
| 月 | 火 | 水 | 木 | 金 | 土 | 日/祝 | |
|---|---|---|---|---|---|---|---|
| 9:00~12:30 |
|
|
|
|
|
~13:00 |
|
| 14:00~17:00 |
|
|
|
|
|
|
|


Please scroll down for the explanation in English.
血尿とは、尿の中に赤血球が混じる状態を指します。目に見えて赤くなる「肉眼的血尿」と、顕微鏡でしか確認できない「顕微鏡的血尿」に分類されます。また、「尿潜血」とは、試験紙を用いた簡易検査で尿中の血液成分(ヘモグロビン)の有無を調べるものです。ただし、尿潜血が陽性でも赤血球が検出されない場合があり、この場合は厳密には血尿とはいいません。これはヘモグロビン尿やミオグロビン尿(筋肉由来)である可能性があります。
血尿を正しく評価するためには、中間尿の採取が原則です。血尿の原因は多岐にわたりますが、大きく「尿路系(非糸球体性)」と「糸球体性」に分類されます。今回は血尿の原因となる疾患をまとめました。各疾患の治療については簡単に触れていますが、別の機会に詳述する予定です。
◆ 尿路系(非糸球体性)血尿
尿路とは腎臓で作られた尿を体外に排出する経路を指します。厳密には非糸球体性血尿と呼称するのが正しいですが、わかりやすいので尿路系血尿とします。尿路(腎盂・尿管・膀胱・前立腺・尿道)の異常が原因の血尿です。特徴としては鮮紅色から暗赤色の血尿が見られ、初尿(出始め)・終尿(終わり)に血尿が多い場合があります。時に血餅(血の塊)が混ざることもあります。
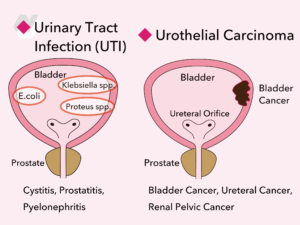
・尿路感染症(膀胱炎・前立腺炎・腎盂腎炎)
最も多いのは膀胱炎による血尿です。頻尿・排尿時痛・残尿感・発熱などの排尿症状を伴い、血尿だけではなく尿混濁も見られるので、診断は比較的容易です。抗菌薬による治療を行います。
・尿路上皮がん
膀胱がん・尿管がん・腎盂(じんう)がんをまとめて尿路上皮がんといいます。男性に多く、喫煙歴はリスクとなります。特に膀胱炎のような排尿症状を伴わずに肉眼的血尿が現れた場合は、尿路のがんを疑う必要があります。超音波検査や尿細胞診、膀胱鏡検査による膀胱内の確認が必要になり、腎盂や尿管がんの可能性がある場合には主にCT検査が行われます。膀胱がんであれば、まず経尿道的手術(内視鏡による膀胱内からの切除)が選択され、深達度によって追加の根治手術が検討されます。腎盂がん・尿管がんがあれば、原則は腎尿管全摘術が根治手術となります。

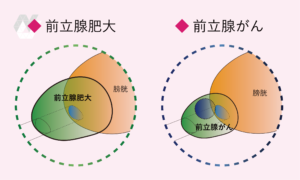
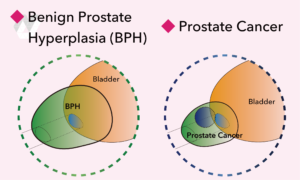
・前立腺疾患(前立腺肥大や前立腺がん)
肥大した前立腺の表面は出血しやすく、基本的には自然に止血されるのを待ちます。前立腺がんは基本的に無症状ですが、血尿の原因となっている場合、がんが進行している可能性があります。診断には超音波検査に加え、以前紹介したPSAの測定が基本となります。必要に応じてMRI検査を追加します。前立腺肥大で出血を繰り返す場合、薬物療法のほかに経尿道的手術も考慮されます。前立腺がんの治療法はステージによって異なり、手術(根治的前立腺全摘術)・放射線治療・ホルモン療法のいずれか、あるいは併用療法を行います。
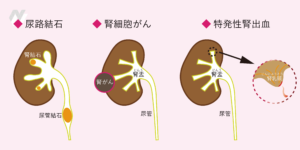
・尿路結石
尿路結石は、腎結石・尿管結石・膀胱結石の総称です。尿管結石は腎疝痛(じんせんつう)として知られる背部から下腹部にかけての激しい痛みを伴うことが多いです。腎結石は無症状のことが多く、膀胱結石では排尿時の痛みや下腹部痛を生じることがあります。小さな結石は自然排出を待ちますが、排出されない場合やサイズが大きい場合は、衝撃波や尿管鏡による破砕手術を検討します。
・腎細胞がん(腎がん)
腎細胞がんも初期の段階では症状がなく、血尿が出る場合には腫瘍のサイズが比較的大きいと考えられます。診断には超音波検査、CT、MRI検査を行います。転移のない腎細胞がんの治療は、原則として手術(根治的腎摘除術ないしは腎部分切除術)です。
・特発性腎出血
かつては原因不明とされていましたが、近年の尿管鏡技術の発達により、腎乳頭の細い血管が破綻して出血していることが明らかになりました。海外では「chronic unilateral hematuria(慢性片側性血尿)」と呼ばれますが、日本では依然として「特発性腎出血」とされています。特に運動後に無症候性の肉眼的血尿が増悪しやすく、若い人にも多いのが特徴です。診断には膀胱鏡でどちらの尿管口から血尿が出ているかを確認し、その後、尿管鏡とレーザーを用いて止血を行います。
◆ 糸球体性血尿
糸球体性血尿は、腎臓の糸球体の異常により、赤血球が尿中に漏れ出ることで生じます。尿の色は赤褐色やコーラ色を呈し、糸球体が障害されているため、尿中には変形赤血球や赤血球円柱が見られるのが特徴で、蛋白尿を伴うことも多いです。
糸球体性血尿の原因として多いのは、慢性糸球体腎炎の一つであるIgA腎症と急性糸球体腎炎です。IgA腎症は上気道感染(風邪や扁桃炎)の後に血尿が出やすいのが特徴で、確定診断には腎生検が必要になることがあります。急性糸球体腎炎は、溶連菌感染(扁桃炎など)の後に発症し、コーラ色の血尿・浮腫・高血圧を伴うことがあります。このほか、自己免疫疾患や血管炎、遺伝性腎疾患(アルポート症候群)なども糸球体性血尿の原因となることがあります。

◆ 最後に
肉眼的血尿や尿潜血を指摘された際に、どこに受診すればよいか迷うことがあるかもしれません。尿路系(非糸球体性)血尿は泌尿器科が専門であり、糸球体性血尿は腎臓内科が専門です。適切に担当科を紹介してもらえるなら、最初は泌尿器科でも内科でも構いません。特に肉眼的血尿が出た場合、尿路悪性腫瘍の可能性もあるため、放置せず早めに受診することをおすすめします。
当院のインスタグラムでも、わかりやすいイラストとともに血尿を解説しております。ぜひご覧ください。ご不明な点があればお気軽にお問い合わせください。
この記事は、西川口泌尿器科クリニック院長 内田裕將(日本専門医機構認定 泌尿器科専門医)により執筆されています。
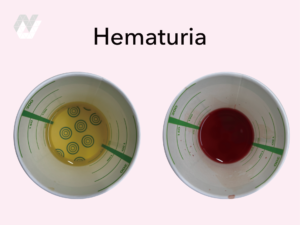
Hematuria refers to the presence of red blood cells in the urine. It is classified into “gross hematuria”, where the urine appears visibly red, and “microscopic hematuria”, which can only be detected under a microscope. Additionally, “urinary occult blood” is a simple test using test strips to check for the presence of hemoglobin in urine. However, in some cases, occult blood tests may be positive even when red blood cells are not detected, which means it is not strictly considered hematuria. This may be due to hemoglobinuria or myoglobinuria, which originates from muscle tissue.
To properly evaluate hematuria, midstream urine collection is the standard method. The causes of hematuria are diverse but can be broadly classified into “urinary tract (non-glomerular)” and “glomerular” origins. This article summarizes diseases that can cause hematuria. While treatments for each condition are briefly mentioned, they will be discussed in detail on another occasion.
◆ Urinary Tract (Non-Glomerular) Hematuria
The urinary tract refers to the pathway through which urine, produced by the kidneys, is excreted from the body. The correct term is non-glomerular hematuria, but for clarity, we will refer to it as urinary tract hematuria. This type of hematuria originates from abnormalities in the urinary tract, including the renal pelvis, ureters, bladder, prostate, and urethra. The characteristic feature is bright red to dark red urine, often more pronounced at the beginning (initial hematuria) or end (terminal hematuria) of urination. Occasionally, blood clots may be present.
・Urinary Tract Infections (Cystitis, Prostatitis, Pyelonephritis)
The most common cause of hematuria is cystitis (bladder infection). It is often accompanied by urinary frequency, dysuria (pain during urination), residual urine sensation, and fever. In addition to hematuria, cloudy urine is also observed, making diagnosis relatively straightforward. Treatment involves antibiotic therapy.
・Urothelial Carcinoma
Bladder cancer, ureteral cancer, and renal pelvic cancer are collectively called urothelial carcinoma. It is more common in men, and a history of smoking is a significant risk factor. If gross hematuria occurs without urinary symptoms like those seen in cystitis, urothelial cancer should be suspected. Diagnostic tests include ultrasound, urine cytology, and cystoscopy for direct visualization of the bladder. If renal pelvic or ureteral cancer is suspected, CT scans are typically performed. For bladder cancer, transurethral resection of the bladder tumor (TURBT) is the initial treatment, and depending on the depth of invasion, additional curative surgery may be considered. In cases of renal pelvic or ureteral cancer, the standard treatment is nephroureterectomy (removal of the kidney and ureter).
・Prostate Disorders (Benign Prostatic Hyperplasia and Prostate Cancer)
An enlarged prostate has a fragile surface prone to bleeding. In most cases, the bleeding stops naturally. Prostate cancer is usually asymptomatic, but if it causes hematuria, it may indicate advanced disease. Diagnosis involves ultrasound and PSA testing, as previously discussed. Additional MRI scans may be performed if needed. For recurrent bleeding due to benign prostatic hyperplasia (BPH), medication or transurethral surgery may be considered. Prostate cancer treatment depends on the stage, including surgery, radiation therapy, or hormone therapy, either alone or in combination.
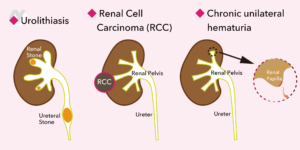
・Urolithiasis
Urolithiasis refers to renal stones, ureteral stones, and bladder stones. Ureteral stones often cause severe pain radiating from the back to the lower abdomen, known as renal colic. Renal stones are often asymptomatic, while bladder stones may cause pain during urination or lower abdominal pain. Small stones may pass naturally, but if they do not or are too large, shock wave lithotripsy (ESWL) or ureteroscopic lithotripsy (URS) may be considered.
・Renal Cell Carcinoma (RCC)
In its early stages, renal cell carcinoma (kidney cancer) is often asymptomatic. If hematuria is present, the tumor is likely to be relatively large. Diagnosis requires ultrasound, CT, and MRI for detailed evaluation. The standard treatment for non-metastatic renal cell carcinoma is either radical nephrectomy or partial nephrectomy.
・Idiopathic Renal Hemorrhage
Previously considered of unknown cause, recent advancements in ureteroscopy have revealed that hematuria often results from ruptured small blood vessels in the renal papilla. While internationally referred to as “chronic unilateral hematuria,” it is still commonly called “idiopathic renal hemorrhage” in Japan. This condition is more common in young individuals and often worsens after exercise. Diagnosis involves cystoscopy to identify the affected ureteral opening (ureteral orifice), followed by ureteroscopy and laser treatment for hemostasis.
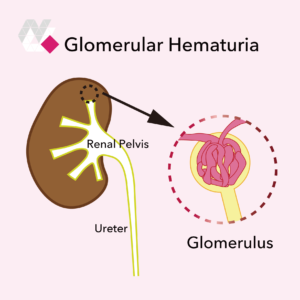
◆ Glomerular Hematuria
Glomerular hematuria occurs due to abnormalities in the glomeruli of the kidneys, allowing red blood cells to leak into the urine. The urine appears brownish-red or cola-colored, and due to glomerular damage, dysmorphic red blood cells and red blood cell casts are often seen in the urine. Proteinuria is also frequently present.
Common causes include IgA nephropathy and acute glomerulonephritis. IgA nephropathy often manifests after upper respiratory tract infections (such as colds or tonsillitis), making hematuria more likely to occur. A kidney biopsy may be necessary for a definitive diagnosis. Acute glomerulonephritis, often caused by streptococcal infections (such as tonsillitis), presents with cola-colored hematuria, swelling (edema), and high blood pressure. Other causes of glomerular hematuria include autoimmune diseases, vasculitis, and genetic kidney disorders (such as Alport syndrome).
◆ Final Note
If you experience gross hematuria or are diagnosed with urinary occult blood, you may wonder which specialist to see. Non-glomerular (urinary tract) hematuria is the domain of urologists, while glomerular hematuria is handled by nephrologists. If a referral can be arranged, visiting either a urologist or a general physician initially is acceptable. However, if gross hematuria is present, there is a possibility of urinary tract malignancies, so early consultation with a specialist is highly recommended.
We also explain hematuria on our Instagram with easy-to-understand illustrations. Please take a look! If you have any questions, feel free to contact us.
This article was written by
Yusuke Uchida M.D., Ph.D.
Director, Nishikawaguchi Urology Clinic
Board-Certified Urologist (certified by the Japanese Medical Specialty Board)